
AFib is a prevelant and growing condition
In the U.S. alone, at least 3-6 million people have non-valvualr atrial fibrillation (AFib), and it's projected to reach over 12 million people by 20301. While AFib management typically begins with antiarrhythmic medications (AADs) and oral anticoagulants (OACs), some patients benefit from both the rhythm control provided by an AFib ablation, as well the freedom from long-term OACs provided by a left atrial appendage closure (LAAC) device.
A dual approach to patient care
Performing an AFib ablation and implanting a WATCHMAN Left Atrial Appendage Closure (LAAC) Device in a single procedural setting offers a comprehensive solution for addressing atrial fibrillation (AFib) progression, rhythm control, and stroke risk reduction. Performing these procedures concomitantly, also known as the FARAWATCH™ approach, not only enhances patient satisfaction by alleviating concerns associated with AFib but also allows patients to avoid multiple procedures and potentially discontinue oral anticoagulation therapy earlier.
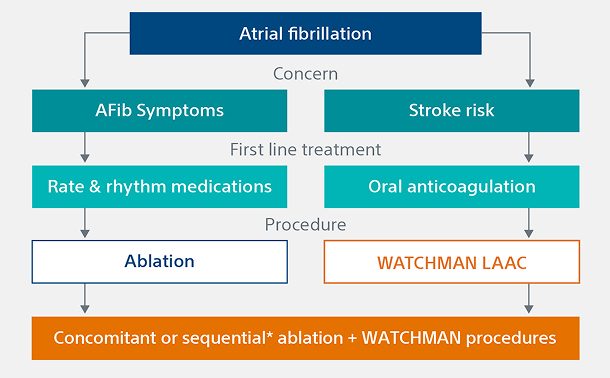
Comparing ablation vs. LAAC treatment options
AFib ablation and LAAC can offer complementary roles in managing AFib. For patients needing rhythm control and/or freedom from oral anticoagulants (OACs), these procedures may provide a comprehensive treatment strategy.
AFib ablation
Address AFib symptoms and achieve rhythm control with multiple ablation modalities, including:

Thermal ablation
Uses extreme heat or cold to create scar tissue and blocks errant electrical signals. This modality may inadvertently affect adjacent tissues.
Pulsed field ablation (PFA)
Utilizes rapid energy pulses to precisely target arrhythmogenic cardiac areas while minimizing collateral tissue damage.
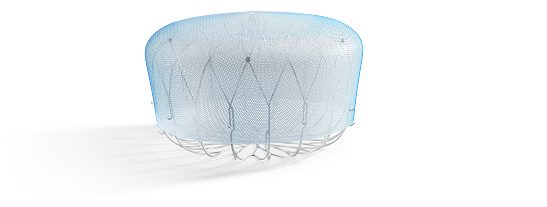
WATCHMAN™ Left Atrial Appendage Closure (LAAC) Implant
The WATCHMAN Implant is a minimally invasive, one-time procedure designed to reduce the risk of strokes that originate in the LAA, offering an alternative to long-term oral anticoagulation therapy and eliminating the risk of long-term OAC-related bleeding complications.
The journey to a combined procedure
As clinical trials broaden AFib patient and treatment indications, clinicians can feel more confident when recommending the WATCHMAN Implant for stroke protection.
WATCHMAN procedure options for comprehensive AFib management
For AFib patients suitable for the WATCHMAN LAAC Device, implanting physicians may suggest one of three procedure options, depending on their eligibility for an AFib ablation and the physician's discretion. Ensure your patients are informed about potential procedure options before their AFib consultation.
 Permanent implant
Permanent implant
Standalone
A WATCHMAN device is implanted in a single procedure.
 Minimally invasive
Minimally invasive
Concomitant
An AFib ablation is performed, and a WATCHMAN device is implanted in a single procedural setting.
 1 day or less average hospital stay
1 day or less average hospital stay
Sequential
An AFib ablation is performed, and a WATCHMAN device is implanted in a later procedure.*
Note: The FARAPULSE PFA Catheter is pictured as representative example for AFib ablation, though any modality may be used.
Boston Scientific provides two industry-leading solutions to help patients manage AFib symptoms and protect against stroke:

FARAPULSE™ Pulsed Field Ablation System
The world's clinical leader in Pulsed Field Ablation (PFA), supported by the world's largest safety registry.2 Treats rate and rhythm symptoms in AFib patients with minimal risk of post-procedural complications.

The WATCHMAN Implant
As the most-studied and implanted LAAC device globally, WATCHMAN delivers a lifetime of stroke protection, without the bleeding risks associated with long-term OAC therapy.
See WATCHMAN clinical evidence
WATCHMAN FLX is an FDA approved device being studied for an expanded indication as a first line therapy vs NOAC for NVAF patients. The use of WATCHMAN or WATCHMAN FLX as a first-line therapy for stroke risk reduction in NVAF patients is considered investigational.
*In the OPTION trial, sequential LAAC was a minimum of 90 days (as a protocol-driven blanking period) and less than 6 months post-AF ablation.
†Thermal AFib ablation only.
References
- Benjamin, EJ et al., Heart Disease and Stroke Statistics—2018 Update: A Report From the American Heart Association. Circulation. 2018. https://doi.org/10.1161/CIR.000000000000055
- Ekanem E, Neuzil P, Reichlin T, et al. Safety of pulsed field ablation in more than 17,000 patients with atrial fibrillation in the MANIFEST-17K study. Nat Med. 2024;30:2020–2029. https://doi.org/10.1038/s41591-024-03114-3